

For years, we’ve been told to “eat real food.” It sounds simple, but the real challenge is figuring out what that actually means—and how official guidelines define it. With the release of the new 2026 Dietary Guidelines, there’s been a surprising shake-up. I went into this expecting the worst. But as it turns out, I may have been wrong. Some parts of these new recommendations are genuinely encouraging—others, not so much.
Let’s break down what the new guidelines get right, where they go wrong, and what it all means for your health.
Table of Contents
- What’s This About a New Pyramid?
- The Good Aspects of the New Guidelines
- Problems With the New Guidelines
- References
What’s This About a New Pyramid?
It feels like South Park has become real. The food pyramid has been inverted in the new dietary guidelines.

And while I was initially worried that these new guidelines would be a disaster, I’m pleased to report that there are some very encouraging aspects—and my worst fears were wrong. Equally, though, it’s not all roses.
The Good Aspects of the New Guidelines
Let’s start with what’s gone right, then we’ll have a look at what’s less ideal. Every new iteration of the dietary guidelines should build upon and improve what’s come before.
The original food pyramid had major issues, such as being too grain-heavy and minimizing healthy unsaturated fats like extra-virgin olive oil [1].

So in 2011, it was scrapped for MyPlate, which was a huge improvement [2].

These new 2026 guidelines don’t replace the old food pyramid. This is a really important point. They replace MyPlate.
MyPlate focused on whole, unprocessed foods, and these new guidelines build upon that base and keep whole foods as their focus.
We can see this clearly in the introduction to the guidelines. The central message is: Eat real food. The guidance goes on to say that we should prioritize whole, nutrient-dense foods and whole grains [3].
Whole grains? What do you mean? The new guideline diagram has whole grains at the bottom, where it looks like we should be minimizing them. So should we be prioritizing whole grains or reducing our intake? More on that shortly, because that’s something that hasn’t gone right.
Coming back to what has gone right: one aspect that wasn’t given enough attention in the MyPlate guidelines was protein intake. Its protein guidance was based on the RDA of 0.8 g/kg/day [4].
But is that really an adequate amount?
You’ve probably noticed the trend. We keep hearing we need to get more protein. Protein shakes, bars, and snacks are everywhere. So is that 0.8 number too low?
There are several reasons higher protein intake can benefit our health.
For instance, muscle mass is a key concern as we get older. We start to lose muscle as early as our 30s, and the loss accelerates with age—particularly during times of illness and bed rest. Muscle mass can decrease by as much as 50% between the ages of 40 and 80. Strength is connected to mass and drops rapidly, too [5].
This is serious. These declines reduce mobility, diminish quality of life, and can lead to fall-related injuries that require costly hospitalization and extended rehabilitation [6].
The crucial question is whether 0.8 g/kg/day is enough to maintain and rebuild muscle mass as we age. An international group of experts has urged a higher target of 1.0 to 1.2 g/kg/day for healthy individuals over 65 [5].
And the evidence supports this. In one observational study, older adults (aged 70–79) who consumed around 1.1 g/kg/day lost 40% less lean body mass over 3 years compared to those eating closer to 0.8 g/kg/day [5].
And since muscle loss begins early, it would make sense to raise protein intake when we’re younger, to a level that maximizes muscle gains.
What Should You Actually Be Eating?
Whole foods vs. supplements — the answer depends on your diet, blood tests, and health goals. Get personalized nutrition recommendations.
Get Your Personalized Health PlanFor muscle building, you’ll often hear 1.6 g/kg/day as a target. That might be high for most people. But a newer meta-analysis found a strong effect up to about 1.3 g/kg/day. Beyond that, benefits plateaued [7].
There’s even a modest weight loss benefit from higher protein intake. One meta-analysis found that studies showing this benefit used protein intakes ranging from 1.07 to 1.6 g/kg/day [8].
Even the low end of that range is well above 0.8 g/kg/day.
And this is where the new guidelines get it right. They recommend 1.2–1.6 g/kg/day, significantly higher than the 0.8 in previous guidelines. They also recognize that needs vary based on age

The new guidelines also continue past advice to vary our protein sources. We need a variety, including animal sources as well as things like beans, nuts, and seeds [3].
There are many other things in the new guidelines that are basically the same as what we’ve seen before. We’re told to eat a variety of colorful, nutrient-dense vegetables and fruits [3].

We should avoid sugar-sweetened drinks and added sugars [3].

And we should keep sodium intake below 2,300 mg/day [3].

Problems With the New Guidelines
But there are three places where the new dietary guidelines have problems.
1. Confusing Guidance on Fats
This is an area where there was a lot of speculation before the guidelines were released. Many expected that they would remove any language warning against saturated fats. At the press conference announcing the new guidelines, RFK Jr. declared they were “ending the war on saturated fats” [9].

In the scientific report published along with the new guidelines, there’s an extensive discussion of the evidence about saturated fats. It argues we don’t have good evidence that lowering saturated fat consumption lowers heart disease risk [10].
And then there’s the appendices, which include a new meta-analysis on saturated fat and heart disease. It specifically challenges the 10% calorie limit that was part of previous guidelines [11].
And that 10% figure was indeed used in the prior 2020 guidelines [12].
So what do the new guidelines actually say? This is where it gets confusing. Despite all of this, the guidelines retain the guidance that we should limit saturated fat to no more than 10% of daily calories [3].

At the same time, the emphasis has clearly shifted. The guidelines say sources of “healthy fats” include meats — which we should probably hear as red meat here, since poultry and seafood are also listed. They also suggest butter and beef tallow as options when cooking [3].

Red meat, butter, and beef tallow are all high in saturated fats. They definitely weren’t recommended in previous guidelines. And mainstream health advice is to limit our consumption of these.
The guidelines also recommend full-fat dairy [3]. This is another departure. The previous guidelines consistently recommended low-fat dairy products [12].

The reason for that earlier recommendation was to avoid saturated fats.
So we can see some evidence of Kennedy’s claim to end the war on saturated fat showing up here in the guidelines. Red meat, butter, beef tallow, and full-fat dairy are all encouraged.
But this is in tension with the 10% guidance. If we’re centering our meals on animal-based proteins and frying stuff in beef tallow, it’s going to be really easy to blow past that threshold. It’s almost like the guidelines can’t make up their mind. Should we limit saturated fats, or shouldn’t we? The overall picture is confusing.
2. Inconsistent Methodology
The second issue has to do with methodology. Because it doesn’t look like they are applying it consistently.
In the scientific report, they lay down a rigorous standard for evidence. They say we need to prioritize randomized, controlled trials over observational studies. Observational studies don’t let us make conclusions about causes—they only uncover potential relationships. Randomized controlled trials give us much greater confidence that we understand what’s going on [10].

When we’re dealing with dietary guidelines, the stakes are high. They can have a profound impact on the food system and on dietary habits across a population. So we want our recommendations to be grounded in the strongest possible evidence [10].
The report also says they will focus on actual clinical outcomes, instead of surrogate markers. In other words, they want to measure how a dietary change affects rates of heart disease—not just blood cholesterol levels. The reason is that changes in these surrogate markers don’t always map onto changes in clinical outcomes in the way we might expect [10].
The authors don’t dismiss observational studies or surrogate markers. They say they have their place. But they want to anchor dietary guidance in experimentally tested relationships whenever available, using other kinds of evidence for context [10].
This emphasis on randomized controlled trials and clinical outcomes is why they find the evidence on saturated fat unconvincing [11].
But then it looks like a different story when it comes to highly processed foods. As we’ve seen, warning against this kind of food is a major theme in the new guidelines.
Does that mean we should avoid protein powders? Plain Greek yogurt? Canned beans or lentils?
And there’s another problem. With such a strong warning against processed foods, you might expect we have good randomized controlled trials focused on clinical outcomes. But the meta-analysis prepared as part of the scientific foundation admits this isn’t the case. Instead, it says the evidence base is almost entirely observational [11].
All of this is a good illustration of how the assumptions we bring to the data will have a significant impact on the conclusions we ultimately draw. If the authors started with a suspicion of saturated fat—that it was guilty until proven innocent—then their recommendations might have gone in a very different direction.
3. The New Food Pyramid Graphic
Let’s move on to one last issue with the new guidelines: the inverted pyramid graphic itself.
The original pyramid was abandoned in 2011 partly because it gave a distorted view of healthy eating. This new pyramid runs a similar risk.
Visually, the image is dominated by a huge steak, a massive chunk of cheese, ground beef, and a whole chicken. There’s a lot of saturated fat represented here, and the portion sizes seem inflated. In contrast, super-healthy plant-based protein sources like chickpeas and lentils are nearly invisible. That’s a pile of beans on top of a bowl of rice, but it would be easy to miss it [3].

And it misrepresents what’s actually in the guidelines. Whole grains occupy a tiny slice at the bottom, despite the recommendation being 2–4 servings a day—roughly the same as in the MyPlate guidelines. Nothing has really changed here [3].

Finally, just like with the older pyramid, this graphic isn’t super helpful for knowing what a balanced healthy meal actually looks like. “Eat real food” is a great slogan. But the challenge comes in knowing which real foods to eat, in what proportions.
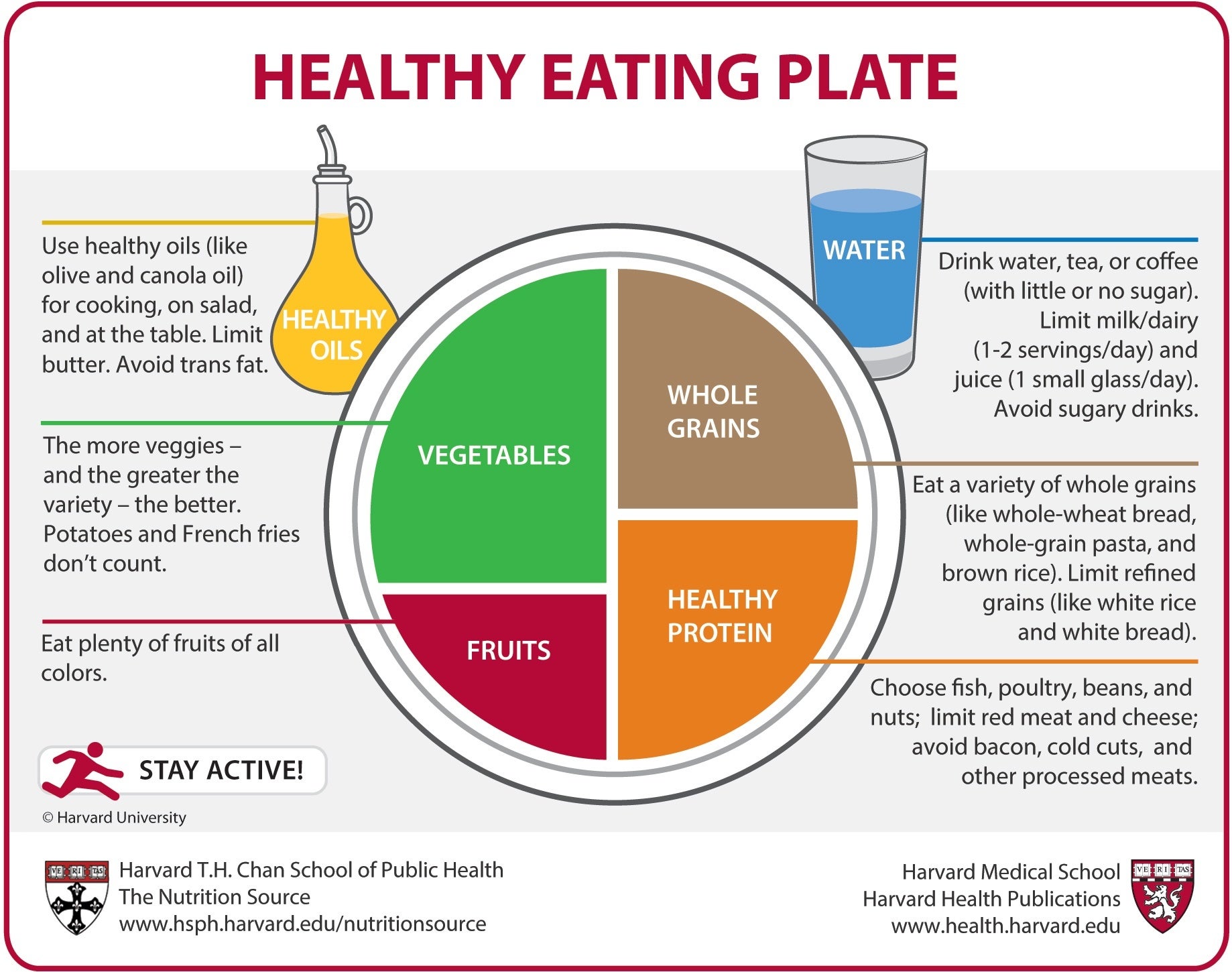
What I steer my patients toward instead is Harvard’s Healthy Eating Plate. It’s similar to MyPlate, but with some updates. It specifies “whole grains” and “healthy” proteins, and includes healthy oils like olive oil [13].

Visually, it’s easy to see what a balanced meal actually looks like on your plate.
Canada’s food plate is another fantastic visual example that’s easy to explain to patients in the clinic [14].

What Should You Actually Be Eating?
Whole foods vs. supplements — the answer depends on your diet, blood tests, and health goals. Get personalized nutrition recommendations.
Get Your Personalized Health PlanReferences
1. https://www.britannica.com/science/food-pyramid
2. https://www.myplate.gov/resources/graphics/myplate-graphics
3. https://cdn.realfood.gov/DGA.pdf
4. https://pmc.ncbi.nlm.nih.gov/articles/PMC5347101/
5. https://pmc.ncbi.nlm.nih.gov/articles/PMC5872778/
6. https://pmc.ncbi.nlm.nih.gov/articles/PMC6442923/
7. https://pmc.ncbi.nlm.nih.gov/articles/PMC7727026/
8. https://pmc.ncbi.nlm.nih.gov/articles/PMC7539343/
9. https://youtu.be/8OqPdybG7eo?t=418
10. https://cdn.realfood.gov/Scientific%20Report_1.8.26.pdf
11. https://cdn.realfood.gov/Scientific%20Report%20Appendices_1.8.26.pdf
13. https://nutritionsource.hsph.harvard.edu/wp-content/uploads/2012/09/HEPJan2015.jpg






{kind=link}